












KAMPALA — A rapidly expanding outbreak of the rare Bundibugyo strain of Ebola has become one of the largest in history, prompting an international public health emergency and an unprecedented race to develop the world’s first vaccine against the virus.
Health authorities in the Democratic Republic of the Congo have confirmed more than 1,150 cases and over 300 deaths, while Uganda has also reported infections linked to the outbreak.
Imported cases involving medical evacuations to Europe and the United States have highlighted how infectious disease outbreaks can quickly become matters of international concern in an era of global travel.
The World Health Organization (WHO) has designated the outbreak a Public Health Emergency of International Concern (PHEIC), its highest level of global health alert. The designation is intended to mobilize international coordination, funding and surveillance rather than signal that widespread global transmission is inevitable.
Ebola is a severe viral hemorrhagic disease caused by viruses in the Ebolavirus family.
It spreads through direct contact with the blood or other bodily fluids of an infected person or contaminated materials and can cause sudden fever, severe weakness, vomiting, diarrhea and, in some patients, internal and external bleeding.
Although some Ebola species have fatality rates approaching 90% in past outbreaks, the Bundibugyo strain has historically been less lethal but remains highly dangerous, particularly because no licensed vaccine or approved treatment currently exists specifically for it.
Unlike respiratory viruses such as SARS-CoV-2, the virus responsible for COVID-19, Ebola does not spread through the air during everyday interactions.
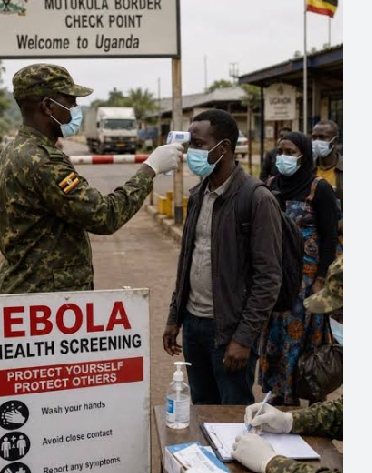
Transmission typically requires close physical contact with an infected person or contaminated bodily fluids, making outbreaks easier to contain when infections are identified quickly through isolation, contact tracing and safe burial practices. However, delayed detection, weak health systems and population movement can allow outbreaks to grow rapidly.
The current epidemic has spread across several provinces in eastern Democratic Republic of the Congo, with Ituri Province accounting for the overwhelming majority of confirmed infections.
Additional cases have been reported in North and South Kivu, while Uganda has recorded infections connected to the cross-border spread of the virus.
Scientists say the outbreak presents a unique challenge because it is caused by Bundibugyo virus rather than the more common Zaire ebolavirus, the strain responsible for most of the world’s largest Ebola epidemics.
Existing Ebola vaccines, including those successfully deployed during previous outbreaks, were developed against the Zaire strain and have not been approved for Bundibugyo virus.
The absence of an approved vaccine has prompted an accelerated international research effort.
The Coalition for Epidemic Preparedness Innovations (CEPI), working with governments and research institutions, has launched parallel development of three vaccine candidates using different technologies, including mRNA, recombinant viral vectors and adenovirus platforms.
The strategy reflects lessons learned during the COVID-19 pandemic, when unprecedented investment and global collaboration enabled vaccines to be developed in record time.
The outbreak has also revived broader questions about global preparedness for emerging infectious diseases. Public health experts note that several pathogens, including Ebola, Zika and mpox, received limited international attention until they expanded beyond their initial hotspots.
COVID-19 exposed how rapidly local outbreaks can disrupt global health systems, economies and international travel, prompting governments to invest more heavily in disease surveillance and pandemic preparedness.
While Ebola poses a very different public health challenge from COVID-19, the current outbreak serves as another reminder that infectious diseases do not respect national borders.
Modern air travel, cross-border trade and humanitarian movement mean that outbreaks in remote regions can quickly demand international attention, even if widespread global transmission remains unlikely.
Health officials stress that the immediate risk to the general public outside affected areas remains low.
The imported cases reported in Europe and the United States involved controlled medical evacuations and strict isolation procedures rather than community transmission. Nevertheless, WHO and national health agencies continue to strengthen surveillance, support frontline healthcare workers and coordinate cross-border response measures to prevent further spread.
For now, containment efforts continue to rely on the traditional pillars of Ebola control: rapid identification of cases, intensive contact tracing, infection prevention in healthcare settings, community engagement and safe, dignified burials.
At the same time, researchers are working to determine whether one of the experimental vaccines can be deployed before the outbreak expands further.
The outbreak has become a critical test of the global health system established after COVID-19. Whether the international community can contain the virus while simultaneously developing a new vaccine may shape future responses to emerging infectious diseases that, like Bundibugyo virus, have long remained outside the world’s scientific spotlight.

















